A 68YRS WITH ALTERED SENSORIUM UNDER EVALUATION SECONDARY TO ?SEPTIC ENCEPHALOPATHY WITH TYPE 2DM SINCE 25YRS WITH HTN SINCE 20YRS WITH LEFT 3RD TOE NON HEALING ULCER
This is an online Elog book to discuss our patient deidentified health data shared after taking his/ her guardians signed informed consent.
Here we discuss our individual patient problems through series of inputs from available Global online community of experts with an aim to solve the patients clinical problem with current best evidence based input.
This Elog also reflects my patient centered online learning portfolio.
I have been given this case to solve in an attempt to understand the topic of “patient clinical data analysis” to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations, and come up with a diagnosis and treatment
Chief complaints::
A 68yr Rtc bus driver came with
C/o ulcer over the left foot since 1month
Blackish discolouration of left 3rd toe since 15days
Burning micturition since 15days
Altered sensation since 3days
History of present illness::
Patient was apparently asymptomatic 1month ago then he had developed pain in left foot region ,insidious in onser gradually progressive ,relieved upon hanging leg along bedside
Next patient developed BLISTER (white coloured) over 3rd toe 1month ago ,it ruptured eventually with very scanty discharge and developed to ulcer presented over pulp of 3rd toe ,for which patient treated by local rmp .
Then patient developed blackish discoloration over left 3rd toe associated with pricking type of pain ,continous type ,radiating towards left leg since 2 days.
H/o burning micturition since 15 days
No H/o Trauma /exposure to severe cold or hot temperature
No h/o fever,vomitings ,loose stools ,pain abdomen ,giddiness
C/o altered sensorium since 3days H/o irrelevent talk,not able to recognize adults
Past history::
Known case of DM -2 since 25yrs on Human mixtard 10u od
K/c/o HTN wince 20yrs on Tab.Telma -H po/od
H/o similar complaints 12yrs ago
Not a known case of TB,cva,cvd,thyroid disorders,epilepsy
Family history::
Not significant
Personal history::
Diet: mixed
Sleep :: adequate
Appetite:: normal
Bowel and bladder:: regular
Addictions::Nil
General examination::
After taking consent patient examined in a well lit room
Patient was conscious coherent cooperative
Well oriented to time ,place ,person
Moderate built, nourishment moderate
pallor present
No icterus
No Lymphadenopathy
No cyanosis
No clubbing
No Edema
Vitals
Temperature::99.3f
PR-110bpm
Bp-150/90 mmhg
RR--18cpm
Local examination::
Blackish discolouration of left 3rd toe
Line of demarcation present
Redness over dorsum of foot left foot present
Skin appears to be shiny,thin and edematous upto ankle region
On palapation::
Local rose of temp present over left leg
Tenderness present over dorsum of left foot upto below knee region
Wet gangrene of left 3rd toe present
No crepitus,no active discharge
All movements normal
Peripheral pulsation::
Right. Left
Dpa. +. +
Ata. +. +
Pta. +. +
Popliteal artery +. +
DISARTICULATION OF LEFT 3rd TOE


Respiratory system::
Inspection::
B/L symmetrical
Trachea appears to be central
Supraclavicular and infraclavicular hallowing absent
Expansion of chest equal on both sides
No crowding of ribs
No drooping of shoulder
Wasting of muscles absent
No scoliosis ,kyphosis
No sinuses,scars,engorged veins
Palpation::
No local rise of temperature
All inspectory findings confirmed
Trachea central
Apex beat felt in 5th ICS in mid clavicular line
Percussion::
Direct : over clavicle and manubrium sternum
Indirect ::::Resonant
Auscultation::
B/L air entry present
On auscultation:: NVBS heard
Inspection..
Shape of abdomen...scaphoid
Umbilicus..inverted,central located
No sinuses or scars on abdomen
Palpation::
No rise in temperature
No Tenderness present
No palpable mass
No free fluid
Liver not palpable
Spleen not palpable
Percussion::
Dull note on right upper quadrant
No fluid thrill
No shifting dullness
Auscultation::
Bowel sound heard:
Cardio vascular system:
Jvp -not raised
Apex beat felt in 5th ICS in mid clavicular line
S1s2 heard
No murmurs
Central nervous system::
Gcs E4V5M6
Power Rt. Lt
ul. 5/5. 5/5
Ll. 5/5. 5/5
Tone N. N
ul. N. N
Ll. N N
Reflexes
Biceps. 2+. 2+
Triceps. 1+. 1+
Supinator. 1+. 1+
Knee 2+. 2+
Ankle 1+. 1+
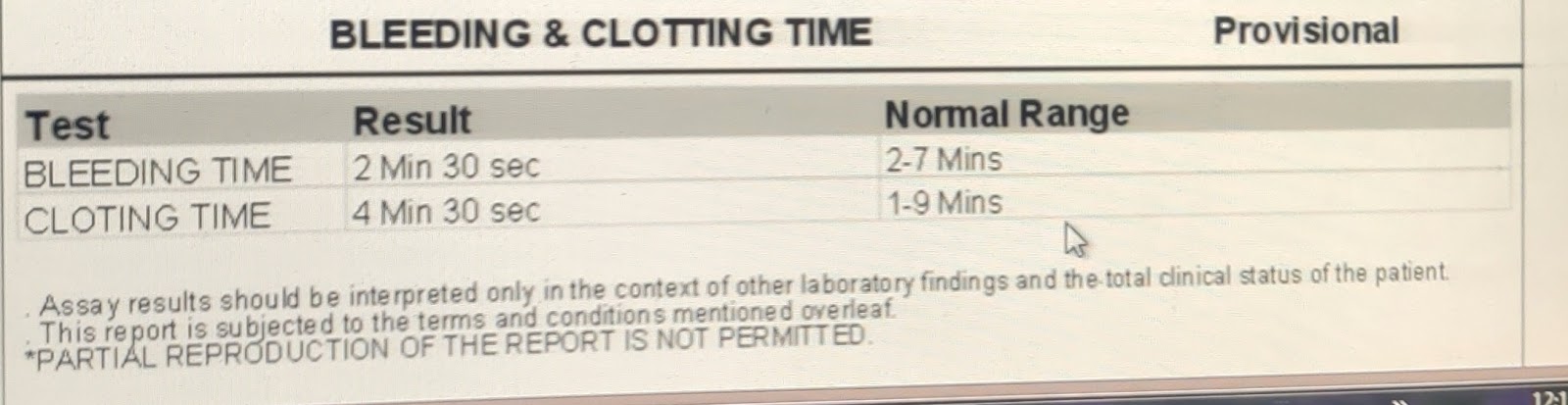
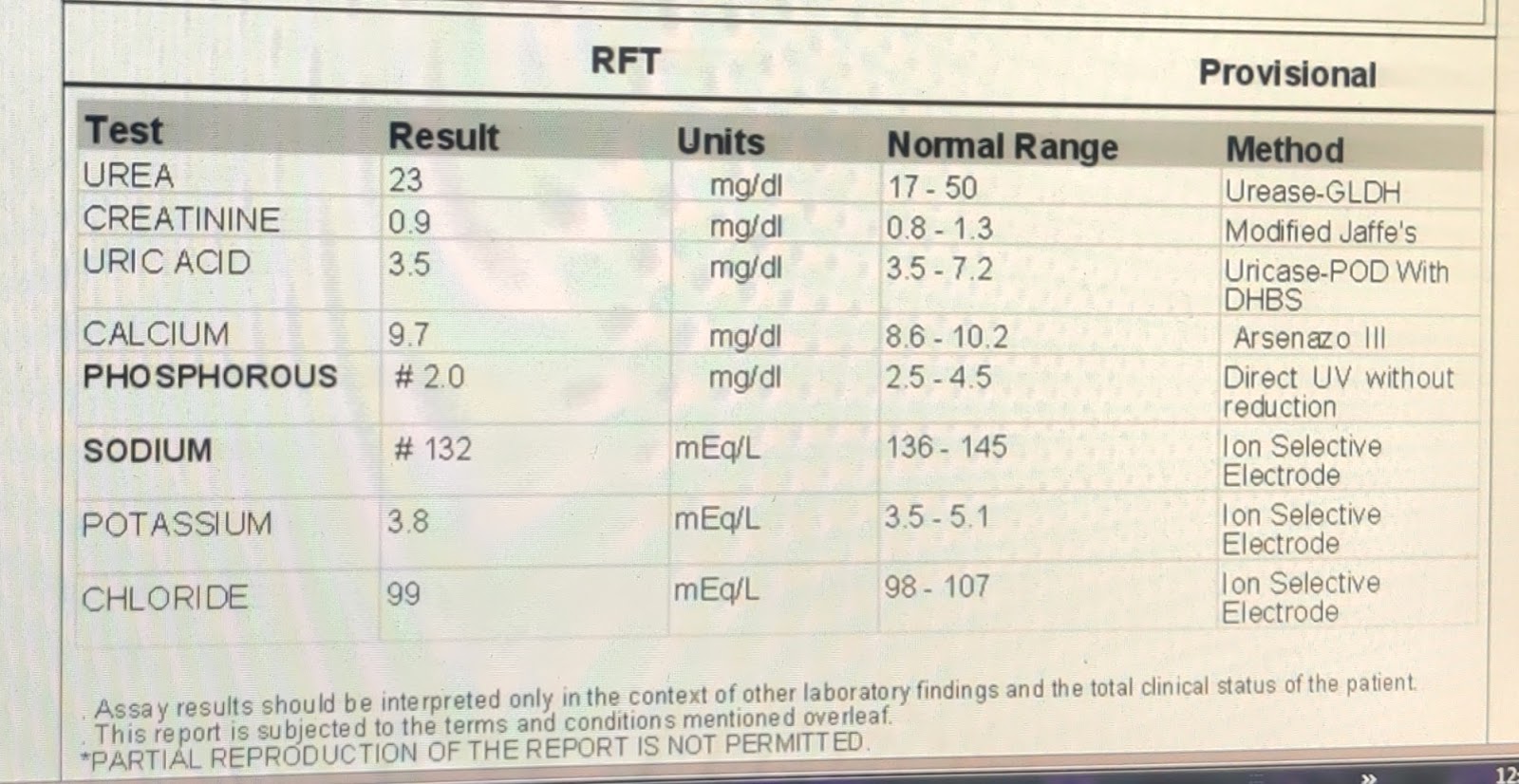
Investigations::
Chest xray PA view ::

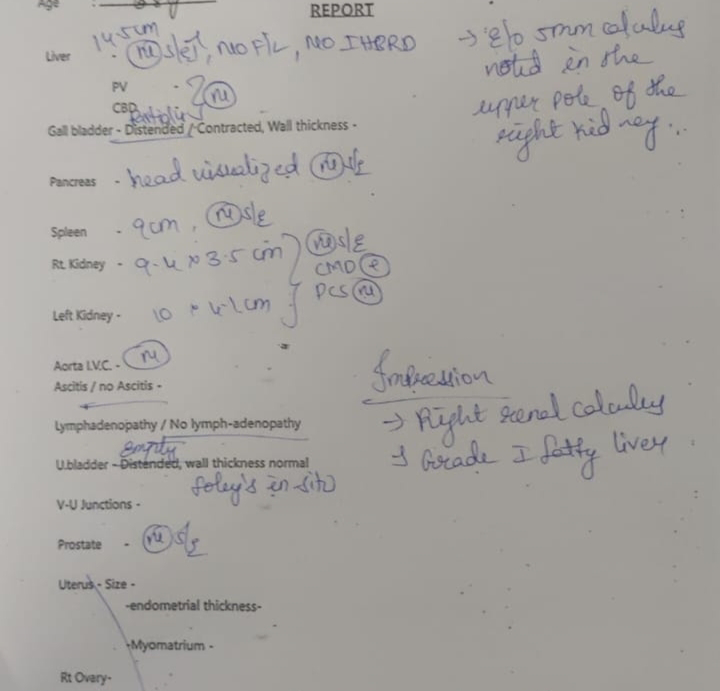
Usg abdomen and pelvis ::






Provisional diagnosis::
ALTERED SENSORIUM UNDER EVALUATION SECONDARY TO ?HYPOGLYCEMIA?SEPSIS WITH TYPE 2DM SINCE 25YRS WITH HTN SINCE 20YRS WITH LEFT 3RD TOE NON HEALING ULCER



Comments
Post a Comment