38 YR OLD WITH SHORTNESS OF BREATH AND PEDAL EDEMA
This is an online Elog book to discuss our patient deidentified health data shared after taking his/ her guardians signed informed consent.
Here we discuss our individual patient problems through series of inputs from available Global online community of experts with an aim to solve the patients clinical problem with current best evidence based input.
This Elog also reflects my patient centered online learning portfolio.
I have been given this case to solve in an attempt to understand the topic of “patient clinical data analysis” to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations, and come up with a diagnosis and treatment
Chief complaints::
A 38 yr old chef by occupation came to casuality with
Shortness of breath since 1 month
Pedal edema since 1month
Decreased urine output since 1month
History of present illness:::
Patient was apparently asymptomatic 1month back then he developed shortness of breath
SHORTNESS OF BREATH which was insidious in onset gradually progressive
Grade 2-3 according to MMRC associated with orthopnea , no paroxysmal nocturnal dyspnoea,no postural and diurnal variation ,no aggrevating or relieving factors
Pedal edema was insidious in onset gradually progressive pitting type from ankle to shin of tibia associated with decreased urine output and facial puffiness
H/o fever -low grade ,intermittent ,no chills and rigor,associated with burning micturition
No nausea,vomiting,loose stools
H/o cough since child hood (k/c/o bronchial asthma) cough was productive with sputum scanty whitish yellow ,no blood tinged,no foul smelling,no postural or diurnal variation
Past History:
-K/c/o Bronchial asthma since childhood
-H/o herniotomy 7yrs back
-H/o sob after herniotomy was managed symptomatically
-H/o chest pain 1yr back and he diagnosed as bronchectasis under acute infective exacerbation with respiratory failure on o2 support with cor pulmonale with Mod
-For which Home oxygen used at 2lt/min via nasal prongs
-H/o pulmonary Tuberculosis in childhood
-Not a k/c/o HTN,DM,epilepsy,CAD,Thyrood disorders
Family history::
Not significant
Personal history::
Diet:mixed
Sleep :: not adequate
Appetite:: decreased
Bowel and bladder:: irregular
Addictions::no addictions
General examination::
After taking consent patient examined in a well lit room
Patient was conscious coherent cooperative
Well oriented to time ,place ,person
Moderate built, nourishment moderate
No pallor
No icterus
No Lymphadenopathy
No cyanosis
No clubbing
Edema present -pitting type
Vitals
Temperature::98.3f
PR-88bpm
Bp-100/70 mmhg
RR--18cpm
Local examination::


Respiratory system::
Inspection::
B/L symmetrical
Trachea appears to be central
Supraclavicular and infraclavicular hallowing absent
Expansion of chest equal on both sides
No crowding of ribs
No drooping of shoulder
Wasting of muscles absent
No scoliosis ,kyphosis
No sinuses,scars,engorged veins
Palpation::
No local rise of temperature
All inspectory findings confirmed
Trachea central
Apex beat felt in 6th ICS in mid clavicular line
Percussion::
Direct : over clavicle and manubrium sternum
Indirect ::::
RT. LT .
Supraclavicular. Resonant. Resonant
Infraclavicular. Resonant. Resonanat
Mammary. Resonant. Dullness
Axillary Resonant. Resonant
Infraaxillary. Resonant Resonant
Suprascapular. Resonant. Resonant
Interscapular. Resonant Resonant
Infrascapular. Resonant Resonant
Auscultation::
B/L air entry present
On auscultation:: Diffuse Crepts are heard (more prominent over bilateral infra clavicular, infrascapular,suprascapular,infra axillary ,mammary area )
Inspection..
Shape of abdomen...scaphoid
Umbilicus..inverted,central located
No sinuses or scars on abdomen
Palpation::
No rise in temperature
No Tenderness present
No palpable mass
No free fluid
Liver not palpable
Spleen not palpable
Percussion::
Dull note on right upper quadrant
No fluid thrill
No shifting dullness
Auscultation::
Bowel sound heard:
Cardio vascular system:
Jvp -Raised
Apex beat felt in 6th ICS in mid clavicular line
S1s2 heard
No murmurs
Central nervous system::
Speech normal
Cranial nerves intact
Sensory and motor system: normal
Reflexes.normal
Investigations::
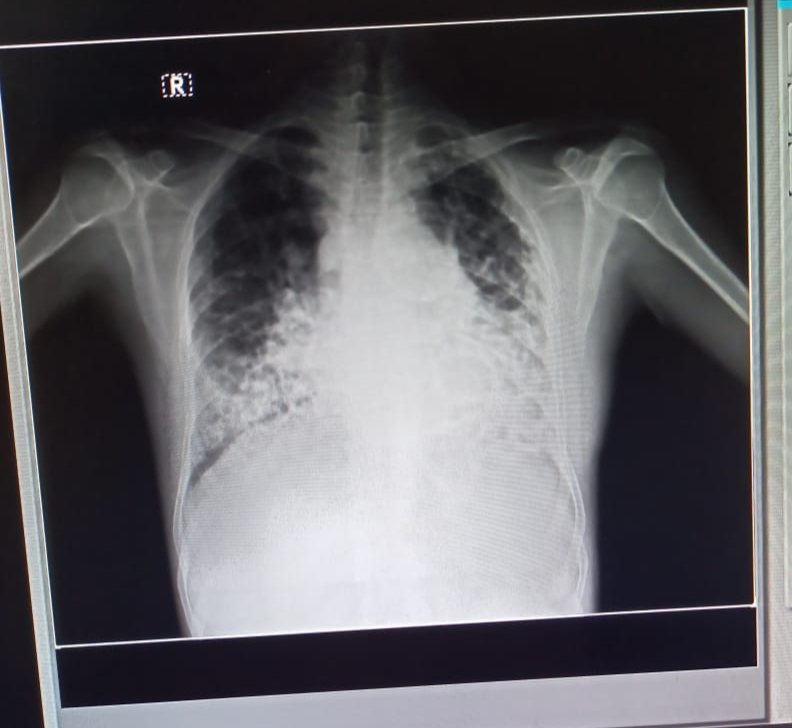
Chest xray PA view::on 22/6/23

23/6/23






Hemogram::
On 23/6/23
Hemoglobin.14.3gm%
Total leucocyte count 14000
Neutrophils 89.7%
Lymphocytes 5.7%
Monocytes 4.6%
Eosinophils 0%
Basophils 0%
Platelet count 73000
Mcv-72
Mch-20
Mchc-28
Rbs-135mg/dl
Complete urine examination::
pale yellow urine
Clear
Rbcs nil
Casts nil
Pus cells-2-3
Epithelial cells 2-3
Liver function tests::on 22/06/23
Total bilirubin:2.4mg/dl
Direct bilirubin:0.35mg/dl
ALP:115 U /L
SGOT:182U /L
SGPT :156 U /L
TotalProteins:7.0g/dl
Albumin-3.1g/dl
Albumin/GlobulinRatio:0.82
RFT
serum creatinine::2.5mg/dl
Uric acid -8.9mg/dl
Urea-38
Phosporus-5.1
Na+::144 mEq/L
K+::3.2mEq/L
Cl-::102mEq/K
calcium::10.1
Serology-
HBSAGRAPID-NEGATIVE
HIV1/2RAPID-NON REACTIVE
ANTI HCV ANTIBODIES- Negative
Usg abdomen on 22/06/23
No sonological abnormalities detected



Investigations 25/6/23 and 26/6/23


Provisional diagnosis::HEART FAILURE (CORPULMONALE) with TYPE 2 RESPIRATORY FAILURE secondary to ?bronchial Asthma with Acute kidney injury secondary to UTI/ATN (MODS)
Treatment::
1.fluid restriction
2.head end elevation
3.o2support to maintain saturation
4.chest physiotherapist
5. Nebulisation budecort



Comments
Post a Comment